
As part of the ordination process, I was required to enroll in Clinical Pastoral Education or CPE for short. The main purpose of CPE is to provide clergy an experience of hospital chaplaincy while at the same time equipping them to be more aware of the psychological impact of ministry. Clinical hours typically take place in a hospital under the supervision of a certified, licensed counselor.
During my program at Duke University Hospital, I was assigned to the Obstetrics & Gynecology floor. The most uncomfortable aspect of my rotation (of which they were a number) turned out to be the weekly discharge meetings with the charge nurse and staff. It was not easy asking questions about hysterectomies to a room full of women. Not a single nurse friended me during those three months (Zuckerberg had not invented Facebook).
During my semester in CPE, the supervisor shared what they considered to be “best practices” for patient rotations. They instructed us on how to enter a room. They even gave us specific directions on who to stand next to in the room. They would ask, “Who do you stand with when you enter a hospital room? The family or the doctor?” And then they answered their question. “You never stand next to the doctor! You always stand next to the family. You are there for the family. If you stand with the doctor, the family will see you as hospital staff, and you will weaken your effectiveness as clergy.” That’s not verbatim (if you have been in CPE, that’s a pun), but it’s close enough. It certainly was one way to deal with triangles in a hospital. At the time, it seemed like a good idea. I lacked enough experience to question this idea that doctors are suspect and patients are deserving.
The directive to stand with family members came out of the supervisor’s experience and frustration. I was unaware at the time of not only the triangle between doctor, patient, and clergy but also I was unaware of the interlocking triangles between my supervisor, nurses, doctors, patients, and other trainees. The supervisor did not elaborate on their problematic past with doctors which is ironic because this is how the CPE program works – recount experiences and feelings. My hunch is the dislike of doctors came out of experiences in which they were pulled aside by nurses and doctors whenever the staff was trying to get the family to agree on a specific course of action. In other words, the doctors and nurses would enlist the clergy person to pile on if the family was resistant or being problematic.
Hospitals are anxious institutions. When families gather under stressful conditions, it can increase chronic levels of anxiety. Each staff person (doctor, nurse, tech, administrator, social worker, etc.) has a level of functioning that is grounded in their family of origin. For those at a higher level of functioning (raised in families with higher levels), they can manage and, in most cases, decrease their level of anxiety. For those at lower levels of functioning (raised in families with lower levels), with a challenged prefrontal cortex to down regulate reactivity, anxiety increases automatically during stressful situations. All of this is to say that families and patients will vary in their capacity to engage anxious situations. Some do better than others.
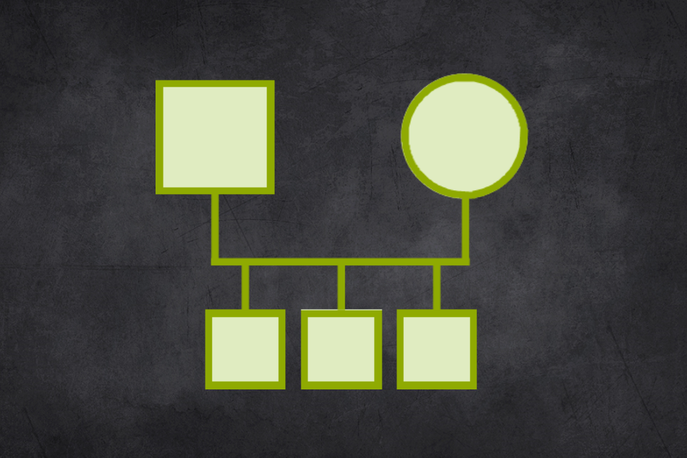
The relationship system helps humans balance out the perceived pressures of anxiety. We do this through the concept of what Dr. Murray Bowen described as the triangle. When two people are anxious, a third person is typically brought in to relieve the tension. The third person takes sides which will put one person of the triangle in an outsider position. Depending on the level of tension between the original twosome, the outsider position is advantages if tension is high. The insider position is desirable when the tension is low. The triangle is the way anxiety travels through the relationship system.
When a patient’s condition is serious, or if the relationship with the doctor is tense, clergy may be unaware they are in a triangle with the patient (perhaps an interlocking triangle which also includes family members) and the doctor. There are several factors or variables that can influence the outcome of anxiety traveling through these triangles.
Things that create tension in a hospital room:
- A doctor who is anxious about giving a patient and family members a prognosis and recommended treatment options.
- A nurse who is uncomfortable providing a specific kind of treatment or care.
- A patient or doctor who struggles to relate to the other based on a bias.
- Conflicting ideas among hospital staff or between patient, family, and doctor about next steps.
- A patient who lacks confidence in choosing a course of action or who needs more information.
- The family leader not being available for a decision.
- A recent birth, death, divorce, or life challenge in the family of the doctor, nurse, or patient.
The medical insurance companies researched why some doctors were more likely to be sued for malpractice and while others were not. The research concluded that it was "bedside manners." Doctors that had good bedside manners did not get sued, even if they made a mistake! What are bedside manners? Excellent question. It's not clear, but there are some vague ideas out there. I think this research says more about the role of anxiety. I'd put my money on the fact that doctors who had better self regulation of their anxious reactivity were able to relate better to their patients and the patients can tell the difference.
If clergy are not thinking triangles, they can easily get caught up in the emotional process between the patient, family, doctor, and nursing staff. If clergy are not aware of their position in these triangles, they may even perpetuate problems. A good leader who is thinking systems can turn a reactive, decision-making process into a more reflective and thoughtful effort with better outcomes.
Clergy are at their best when they stand on their own, taking neither the side of the family nor the doctor. By sides, I’m referring to emotional sides: either trying to take control of a situation or keeping a distance. I can always tell how anxious I am when I either try to tell someone what to do or when I stop engaging someone. By focusing on being more of a self in the hospital room, not taking emotional sides, clergy function better in relationship to both doctor and patient (and family). It requires an effort to regulate one’s anxiety, thinking clearly, and being available to think with anyone who is willing to engage thinking. It involves asking good questions. For example, who has the greatest capacity to think about what is happening and what to do? Who is the decision maker and what does it look like to make a responsible decision?
Inevitably, during a hospital visit, I become aware of how uncomfortable I am. It may happen in reaction to the behavior of the patient or the doctor. It may happen in reaction to a decision or the way someone is treated. If I’m not able to engage my thinking, I can quickly go down the road of blaming others or myself. In these instances, after a few minutes in the car on the way home, I can sometimes pull up enough self to think about where I see this same situation happening in my family. Where are the examples of this problem in my own family? From there I begin the important work of thinking about the family emotional process, how I predictably participate in it, how others predictably participate in it, and what I can do to change my part in the relationship system. Doing this important work allows me to function at a higher level the next time I enter a hospital room.
Over the years, I’ve learned to ask myself these questions before entering a room:
- What is my purpose for this visit? What is my goal? How do I stay the course with my goal?
- What does it mean to be adaptable and flexible during my visit? What am I willing to do and what am I not willing to do?
When I leave, I often ask myself, what have I learned from this visit about relationship systems?
A final word about the word “patient.” Dr. Bowen refused to use this word. In fact, he saw diagnosis as part of the problem. When a person in the family is identified as having a problem (the patient with a diagnosis) everyone in the family calms down. But it is always at the expense of the person who is labeled. Dr. Bowen saw the diagnosis, not as something in the person but, as something in the whole family as a single unit. He even went so far as to say that there was a little bit of schizophrenia in all of us. My use of the word "patient" in this blog post is to identify which person I am talking about in the hospital room. I suppose I could have used words like “perceived patient,” or “the focus of the family projection process,” but I chose to use patient instead. In my day to day work, I do not identify people as a patient or problem. I am less interested in a diagnosis and more interested in the emotional process that leads to someone accepting a diagnosis.


 RSS Feed
RSS Feed